Comparative Health and Medicine
Overview
- Explain the different types of health care available in the United States
- Compare the health care system of the United States with that of other countries
There are broad, structural differences among the healthcare systems of different countries. In core nations, those differences might arise in the administration of healthcare, while the care itself is similar. In peripheral and semi-peripheral countries, a lack of basic healthcare administration can be the defining feature of the system. Most countries rely on some combination of modern and traditional medicine. In core countries with large investments in technology, research, and equipment, the focus is usually on modern medicine, with traditional (also called alternative or complementary) medicine playing a secondary role. In the United States, for instance, the American Medical Association (AMA) resolved to support the incorporation of complementary and alternative medicine in medical education. In developing countries, even quickly modernizing ones like China, traditional medicine (often understood as “complementary” by the western world) may still play a larger role.
U.S. Healthcare
U.S. healthcare coverage can broadly be divided into two main categories: public healthcare (government-funded) and private healthcare (privately funded).
The two main publicly funded healthcare programs are Medicare, which provides health services to people over sixty-five years old as well as people who meet other standards for disability, and Medicaid, which provides services to people with very low incomes who meet other eligibility requirements. Other government-funded programs include service agencies focused on Native Americans (the Indian Health Service), Veterans (the Veterans Health Administration), and children (the Children’s Health Insurance Program). A controversial issue in 2011 was a proposed constitutional amendment requiring a balanced federal budget, which would almost certainly require billions of dollars in cuts to these programs. As discussed below, the United States already has a significant problem with lack of healthcare coverage for many individuals; if these budget cuts pass, the already heavily burdened programs are sure to suffer, and so are the people they serve (Kogan 2011).
The U.S. Census (2011) divides private insurance into employment-based insurance and direct-purchase insurance. Employment-based insurance is health plan coverage that is provided in whole or in part by an employer or union; it can cover just the employee, or the employee and his or her family. Direct purchase insurance is coverage that an individual buys directly from a private company.
With all these insurance options, insurance coverage must be almost universal, right? Unfortunately, the U.S. Census Current Population Survey of 2013 shows that 18 percent of people in the United States have no health insurance at all. Equally alarming, a study by the Commonwealth Fund shows that in 2010, 81 million adults were either uninsured or underinsured; that is, people who pay at least 10 percent of their income on healthcare costs not covered by insurance or, for low-income adults, those whose medical expenses or deductibles are at least 5 percent of their income (Schoen, Doty, Robertson, and Collins 2011). The Commonwealth study further reports that while underinsurance has historically been an issue that low-income families faced, today it is affecting middle-income families more and more.
Why are so many people uninsured or underinsured? Skyrocketing healthcare costs are part of the issue. Many people cannot afford private health insurance, but their income level is not low enough to meet eligibility standards for government supported insurance. Further, even for those who are eligible for Medicaid, the program is less than perfect. Many physicians refuse to accept Medicaid patients, citing low payments and extensive paperwork (Washington University Center for Health Policy, n.d.).
Healthcare in the United States is a complex issue, and it will only get more so with the continued enactment of the Patient Protection and Affordable Care Act (PPACA) of 2010. This Act, sometimes called “ObamaCare” for its most noted advocate, President Barack Obama, represents large-scale federal reform of the United States’ healthcare system. The PPACA aims to address some of the biggest flaws of the current healthcare system. It expands eligibility to programs like Medicaid and CHIP, helps guarantee insurance coverage for people with pre-existing conditions, and establishes regulations to make sure that the premium funds collected by insurers and care providers go directly to medical care. It also includes an individual mandate, which requires everyone to have insurance coverage by 2014 or pay a penalty. A series of provisions, including significant subsidies, are intended to address the discrepancies in income that are currently contributing to high rates of uninsurance and underinsurance. In 2012 the U.S. Supreme Court upheld the constitutionality of the PPACA's individual mandate. According to Blumenthal (2014), 20 million people in the United States have gained health insurance under PPACA. This lowers the number of uninsured people to 13 percent.

The PPACA remains contentious. The Supreme Court ruled in the case of National Federation of Independent Businesses v. Sebelius in 2012, that states cannot be forced to participate in the PPACA's Medicaid expansion. This ruling has opened the door to challenges to the PPACA in Congress and the Federal courts, some state governments, conservative groups and independent businesses. A concern to public health officials is fear among some parents that certain vaccines such as the measels, mumps, and rubella (MMR) vaccine are linked to higher risk of autism. According to Uchiyama et al (2007), there is no link between the MMR and autism. However fear of this perceived link pushes some parents to refuse the MMR vaccine for their children.
An additional issue in U.S. healthcare has been the push to legalize marijuana in some states. As of this writing, twenty-three states and the District of Columbia allow the use of medical cannabis (Borgelt 2013). Marijuana reform appears to partly be the repackaging of marijuana from a drug to a "medicine." Medical evidence has demonstrated positive responses in treatment of a variety of illnesses, from some cancers to glaucoma and epilepsy. Concerns regarding cost and long term effects of the PPACA continue to be discussed at various societal levels.
Healthcare Elsewhere
Clearly, healthcare in the United States has some areas for improvement. But how does it compare to healthcare in other countries? Many people in the United States are fond of saying that this country has the best healthcare in the world, and while it is true that the United States has a higher quality of care available than many peripheral or semi-peripheral nations, it is not necessarily the “best in the world.” In a report on how U.S. healthcare compares to that of other countries, researchers found that the United States does “relatively well in some areas—such as cancer care—and less well in others—such as mortality from conditions amenable to prevention and treatment” (Docteur and Berenson 2009).
One critique of the Patient Protection and Affordable Care Act is that it will create a system of socialized medicine, a term that for many people in the United States has negative connotations lingering from the Cold War era and earlier. Under a socialized medicine system, the government owns and runs the system. It employs the doctors, nurses, and other staff, and it owns and runs the hospitals (Klein 2009). The best example of socialized medicine is in Great Britain, where the National Health System (NHS) gives free healthcare to all its residents. And despite some U.S. citizens’ knee-jerk reaction to any healthcare changes that hint of socialism, the United States has one socialized system with the Veterans Health Administration.
It is important to distinguish between socialized medicine, in which the government owns the healthcare system, and universal healthcare, which is simply a system that guarantees healthcare coverage for everyone. Germany, Singapore, and Canada all have universal healthcare. People often look to Canada’s universal healthcare system, Medicare, as a model for the system. In Canada, healthcare is publicly funded and is administered by the separate provincial and territorial governments. However, the care itself comes from private providers. This is the main difference between universal healthcare and socialized medicine. The Canada Health Act of 1970 required that all health insurance plans must be “available to all eligible Canadian residents, comprehensive in coverage, accessible, portable among provinces, and publicly administered” (International Health Systems Canada 2010).
Heated discussions about socialization of medicine and managed-care options seem frivolous when compared with the issues of healthcare systems in developing or underdeveloped countries. In many countries, per capita income is so low, and governments are so fractured, that healthcare as we know it is virtually non-existent. Care that people in developed countries take for granted—like hospitals, healthcare workers, immunizations, antibiotics and other medications, and even sanitary water for drinking and washing—are unavailable to much of the population. Organizations like Doctors Without Borders, UNICEF, and the World Health Organization have played an important role in helping these countries get their most basic health needs met.
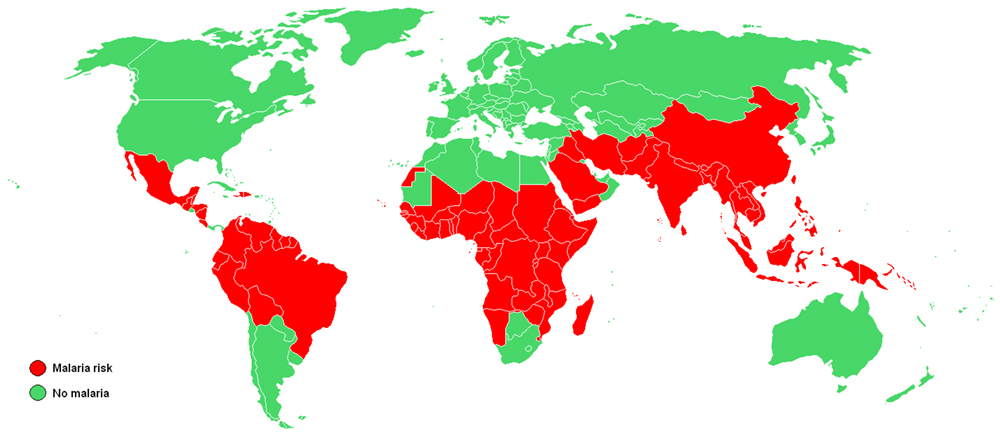
WHO, which is the health arm of the United Nations, set eight Millennium Development Goals (MDGs) in 2000 with the aim of reaching these goals by 2015. Some of the goals deal more broadly with the socioeconomic factors that influence health, but MDGs 4, 5, and 6 all relate specifically to large-scale health concerns, the likes of which most people in the United States will never contemplate. MDG 4 is to reduce child mortality, MDG 5 aims to improve maternal health, and MDG 6 strives to combat HIV/AIDS, malaria, and other diseases. The goals may not seem particularly dramatic, but the numbers behind them show how serious they are.
For MDG 4, the WHO reports that 2009 infant mortality rates in “children under 5 years old in the WHO African Region (127 per 1000 live births) and in low-income countries (117 per 1000 live births) [had dropped], but they were still higher than the 1990 global level of 89 per 1000 live births” (World Health Organization 2011). The fact that these deaths could have been avoided through appropriate medicine and clean drinking water shows the importance of healthcare.
Much progress has been made on MDG 5, with maternal deaths decreasing by 34 percent. However, almost all maternal deaths occurred in developing countries, with the African region still experiencing high numbers (World Health Organization 2011).
On MDG 6, the WHO is seeing some decreases in per capita incidence rates of malaria, tuberculosis, HIV/AIDS, and other diseases. However, the decreases are often offset by population increases (World Health Organization 2011). Again, the lowest-income countries, especially in the African region, experience the worst problems with disease. An important component of disease prevention and control is epidemiology, or the study of the incidence, distribution, and possible control of diseases. Fear of Ebola contamination, primarily in Western Africa but also to a smaller degree in the United States, became national news in the summer and fall of 2014.
References
Anders, George. 1996. Health Against Wealth: HMOs and the Breakdown of Medical Trust. Boston: Houghton Mifflin.
Centers for Disease Control and Prevention. 2014 "Attention Deficit/Hyperactivity Disorder (ADHD) Data and Statistics." Retrieved October 13, 2014 (http://www.cdc.gov/ncbddd/adhd/data.html)
Docteur, Elizabeth, and Robert A. Berenson. 2009. “How Does the Quality of U.S. Health Care Compare Internationally?” Timely Analysis of Immediate Health Policy Issues 9:1–14.
Kaiser Family Foundation. 2011. “Health Coverage of Children: The Role of Medicaid and CHIP.” Retrieved December 13, 2011 ( http://www.kff.org/uninsured/upload/7698-05.pdf ).
Kaiser Family Foundation. 2010. “International Health Systems: Canada.” Retrieved December 14, 2011 ( http://www.kaiseredu.org/Issue-Modules/International-Health-Systems/Canada.aspx ).
Klein, Ezra. 2009. “Health Reform for Beginners: The Difference between Socialized Medicine, Single-Payer Health Care, and What We'll Be Getting.” The Washington Post, December 14. Retrieved December 15, 2011 ( http://www.bloomberg.com/news/2011-12-15/don-t-let-death-panels-kill-a-better-way-to-die-commentary-by-ezra-klein.html).
Kogan, Richard. 2011. “Program Cuts Under a Balanced Budget Amendment: How Severe Might They Be?” Center on Budget and Policy Priorities. Retrieved December 15, 2011 (http://www.cbpp.org/cms/?fa=view&id=3619).
Pear, Robert. 2011. “In Cuts to Health Programs, Experts See Difficult Task in Protecting Patients.” The New York Times, September 20. Retrieved December 13, 2011 (http://www.nytimes.com/2011/09/21/us/politics/wielding-the-ax-on-medicaid-and-medicare-without-wounding-the-patient.html ).
Schoen, C., M.M. Doty, R.H. Robertson, and S.R. Collins. 2011. "Affordable Care Act Reforms Could Reduce the Number of Underinsured U.S. Adults by 70 Percent." Health Affairs 30(9):1762–71. Retrieved December 13, 2011 ( http://www.commonwealthfund.org/Publications/In-the-Literature/2011/Sep/Reduce-Uninsured.aspx ).
Uchiyma, T., M. Kurosawa, Y. Inaba. 2007. "MMR-Vaccine and Regression in Autism Spectrum Disorders: Negative Results Presented from Japan." Journal of Autism and Deviant Disorders 37(2):210–7.
U.S. Census. 2011. “Coverage by Type of Health Insurance: 2009 and 2010.” U.S. Census Bureau, Current Population Survey, 2010 and 2011 Annual Social and Economic Supplements. Retrieved December 13, 2011 ( http://www.census.gov/hhes/www/hlthins/data/incpovhlth/2010/table10.pdf ).
U.S. Census. 2011. “CPS Health Insurance Definitions.” Retrieved December 13, 2011 ( http://www.census.gov/hhes/www/hlthins/methodology/definitions/cps.html ).
Washington University Center for Health Policy. n.d. “Health Care Access for Medicaid Patients—Physicians and Dentists Interview Study.” Retrieved December 15, 2011 ( http://healthpolicy.wustl.edu/Content/HealthCareAccess.html?OpenDocument ).
World Health Organization. 2011. “World Health Statistics 2011.” Retrieved December 12, 2011 ( http://www.who.int/gho/publications/world_health_statistics/EN_WHS2011_Part1.pdf ).
World Health Organization. 2014. "Ebola Virus Disease Fact Sheet, Updated September 2014." Retrieved October 19, 2014 (http://www.who.int/mediacentre/factsheets/fs103/en/).
Further Research
Project Mosquito Net says that mosquito nets sprayed with insecticide can reduce childhood malaria deaths by half. Read more at http://openstaxcollege.org/l/project_mosquito_net
Short Answer Quiz
What do you think are the best and worst parts of the PPACA? Why?
Compare and contrast the healthcare system of the United States with the WHO’s Millennium Development Goals.
Section Quiz
Which public healthcare system offers insurance primarily to people over sixty-five years old?
- Medicaid
- Medicare
- Veterans Health Administration
- All of the above
Hint:
B
Which program is an example of socialized medicine?
- Canada’s system
- The United States’ Veterans Health Administration
- The United States’ new system under the Patient Protection and Affordable Care Act
- Medicaid
Hint:
B
What does the individual mandate provision of the 2010 U.S. healthcare reform do?
- Requires everyone to buy insurance from the government
- Requires everyone to sign up for Medicaid
- Requires everyone to have insurance or pay a penalty
- None of the above
Hint:
C
Great Britain’s healthcare system is an example of ______________
- socialized medicine
- private healthcare
- single-payer private healthcare
- universal private healthcare
Hint:
A
What group created the Millennium Development Goals?
- UNICEF
- The Kaiser Family Foundation
- Doctors Without Borders
- The World Health Organization
Hint:
D
Summary
There are broad, structural differences among the healthcare systems of different countries. In core nations, those differences include publicly funded healthcare, privately funded healthcare, and combinations of both. In peripheral and semi-peripheral countries, a lack of basic healthcare administration can be the defining feature of the system.